+1.310.385.1918 | 8436 W. 3rd St. #800 L.A.
Follow us:
![]()
![]()
![]()
![]()
![]()
+1.310.385.1918 | 8436 W. 3rd St. #800 L.A.
Follow us:
![]()
![]()
![]()
![]()
![]()

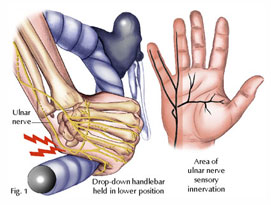
Ulnar nerve compression at the elbow is the second most common nerve entrapment syndrome in the upper extremity. Only carpal tunnel syndrome is seen more frequently. In the region of the elbow, the ulnar nerve passes through a fibromuscular tunnel, the cubital tunnel, as it enters the muscles of the forarm. Elbow flexion causes tightening of this tunnel, resulting in friction, traction and pressure on the ulnar nerve. Chronic compression in this area can cause debilitating symptoms.
Patients often complain of numbness or “pins and needles” sensations involving the small and ring fingers as well as aching of the forearm and elbow. There may also be weakness of the hand resulting in clumsiness, although this is less commonly found. Electrodiagnostic studies (nerve conduction velocities or NCV) are frequently useful for confirming the diagnosis of ulnar nerve entrapment.
Initial treatment in mild or moderate cases can be conservative. The patient is educated about avoiding arm positions that increase compression of the nerve such as prolonged flexion of the elbow. In more severe cases surgery can be considered. Surgical options in general consist of simple decompression of the nerve (excising constricting bands such as the medial intermuscular septum and opening the cubital tunnel) or repositioning the ulnar nerve to a less vulnerable location (nerve transposition). Each technique has specific advantages and disadvantages which one’s surgeon can discuss. Both are highly successful at relieving the symptoms of nerve entrapment.