+1.310.385.1918 | 8436 W. 3rd St. #800 L.A.
Follow us:
![]()
![]()
![]()
![]()
![]()
+1.310.385.1918 | 8436 W. 3rd St. #800 L.A.
Follow us:
![]()
![]()
![]()
![]()
![]()

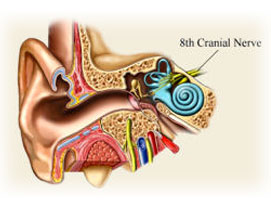
Acoustic neuromas are benign tumors that arise from the Schwann cells that surround the vestibular segment of the vestibulocochlear nerve, the eighth cranial nerve. They are consequently more accurately called “vestibular schwannomas”. These sporadic tumors occur in 2 different patient groups:
1. Patients with no family predisposition or genetic inheritance. These sporadic tumors are invariably located only on one side and are not associated with other tumors or abnormalities within the nervous system.
2.Less commonly a genetic disorder, neurofibromatosis type 2, can lead to acoustic tumors on both sides. In this condition there may be a family history of similar tumors and other intracranial or spinal tumors, such as Meningiomas may be seen as well.
Hearing loss in one ear, usually gradual in onset, is the most common initial symptom. Other symptoms can include ringing in the ear (tinnitus), unsteadiness and dizziness or vertigo. With larger tumors numbness of the face, headache, double vision, poor coordination and difficulty swallowing may be present. The degree of hearing loss, even when subtle, can be documented on audiometric testing. In some cases, there is a decrease in the person’s ability to discriminate between spoken words that are similar sounding, for example “cat” and “hat”.
Magnetic Resonance Imaging (MRI) with intravenous injection of contrast dye can usually establish the diagnosis of acoustic neuroma. Enlargement of the internal auditory canal (the opening in the temporal bone where the facial and vestibulocochlear nerves traverse) may be seen. As the tumor enlarges a round or oval enhancing mass within the posterior fossa can be appreciated. In rare cases, other tumors (most commonly meningiomas) can look similar on MRI, but usually they can be differentiated by recognizing other radiographic features. This is not always possible however.
Alternatives for treatment of acoustic neuromas should be discussed in detail with the treating physician. Most of these tumors are slow growing, although the exact rate of growth is unpredictable in any particular case. Because of the slow growth, when tumors are small and have minimal symptoms, observation with follow-up MRI scans is a reasonable option for some patients, especially when the tumor was found incidentally on an MRI obtained for an unrelated reason. However, when tumors are larger and symptoms are present and the patient is not elderly or debilitated, definitive treatment may be indicated.
Treatment alternatives would include focused radiation therapy, such as stereotactic radiosurgery using the Gamma Knife or the Linear Accelerator. Radiation is a very good option in the elderly patient and those patients who do not wish conventional open surgery. The goal of radiation treatment is to control or stop the growth of the tumors. In some cases the tumor may get smaller, but it is not expected that the tumor will disappear. Hearing preservation can be achieved in many patients. Complications following radiation are rare, but may include radiation injury to adjacent structures such as the brainstem, facial weakness, facial numbness or discomfort, headache, and radiation induced tumors.
Most tumors can be surgically excised. In many cases this is the preferred treatment, especially in patients with larger tumors or when the patient does not desire radiation. Three different surgical approaches have commonly been used. When the tumor is very small, and predominantly located within the internal auditory canal (IAC), a middle fossa approach (surgery above the temporal bone) can be used. In this procedure the bone under the temporal lobe of the brain is exposed and the IAC is opened by drilling bone on the superior surface of the temporal bone. This approach offers the possibility of hearing preservation in some patients. For larger tumors, either the retrosigmoid (surgery behind the temporal bone) or the translabyrinthine (surgery through the temporal bone) approaches are required. Hearing preservation is only possible with the retrosigmoid approach, but a larger exposure of the brain is required. The risks of all surgical procedures include loss of hearing on one side, facial weakness or paralysis, imbalance, leakage of cerebrospinal fluid through the nose, ear or incision, meningitis and other neurologic deficits (eg. stroke, double vision, weakness etc.).
Disruption of the flow of cerebrospinal fluid (CSF) can occur before or after treatment of acoustic neuromas. This results in an increase in pressure within the skull and resultant enlargement of the ventricles (the fluid compartments of the brain). In some cases fluid (CSF) may collect under the scalp following surgery (pseudomeningocele). Treatment of hydrocephalus usually requires placement of a ventriculoperitoneal shunt to divert CSF from the brain into the abdomen.